PDR® entry for
STRATTERA™ (Lilly)
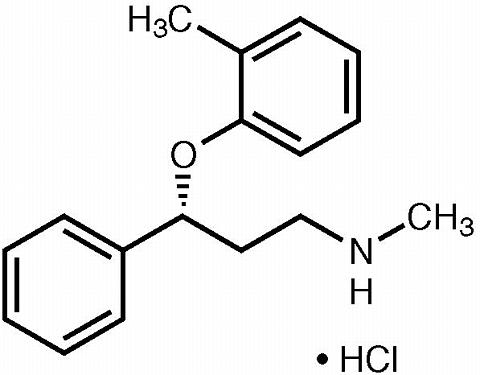
(atomoxetine HCl)
DESCRIPTION
STRATTERA™ (atomoxetine HCl) is a selective norepinephrine reuptake inhibitor. Atomoxetine HCl is the R (-) isomer as determined by x-ray diffraction. The chemical designation is (-)- N -methyl-3-phenyl-3-( o -tolyloxy)-propylamine hydrochloride. The molecular formula is C 17 H 21 NO•HCl, which corresponds to a molecular weight of 291.82. The chemical structure is:
Atomoxetine HCl is a white to practically white solid, which has a solubility of 27.8 mg/mL in water.
STRATTERA capsules are intended for oral administration only.
Each capsule contains atomoxetine HCl equivalent to 10, 18, 25, 40, or 60 mg of atomoxetine. The capsules also contain pregelatinized starch and dimethicone. The capsule shells contain gelatin, sodium lauryl sulfate, and other inactive ingredients. The capsule shells also contain one or more of the following: FD&C Blue No. 2, synthetic yellow iron oxide, titanium dioxide. The capsules are imprinted with edible black ink.
CLINICAL PHARMACOLOGY
Pharmacodynamics and Mechanism of Action
The precise mechanism by which atomoxetine produces its therapeutic effects in Attention-Deficit/Hyperactivity Disorder (ADHD) is unknown, but is thought to be related to selective inhibition of the pre-synaptic norepinephrine transporter, as determined in ex vivo uptake and neurotransmitter depletion studies.
Human Pharmacokinetics
Atomoxetine is well-absorbed after oral administration and is minimally affected by food. It is eliminated primarily by oxidative metabolism through the cytochrome P450 2D6 (CYP2D6) enzymatic pathway and subsequent glucuronidation. Atomoxetine has a half-life of about 5 hours. A fraction of the population (about 7% of Caucasians and 2% of African Americans) are poor metabolizers (PMs) of CYP2D6 metabolized drugs. These individuals have reduced activity in this pathway resulting in 10-fold higher AUCs, 5-fold higher peak plasma concentrations, and slower elimination (plasma half-life of about 24 hours) of atomoxetine compared with people with normal activity [extensive metabolizers (EMs)]. Drugs that inhibit CYP2D6, such as fluoxetine, paroxetine, and quinidine, cause similar increases in exposure.
The pharmacokinetics of atomoxetine have been eva luated in more than 400 children and adolescents in selected clinical trials, primarily using population pharmacokinetic studies. Single-dose and steady-state individual pharmacokinetic data were also obtained in children, adolescents, and adults. When doses were normalized to a mg/kg basis, similar half-life, C max , and AUC values were observed in children, adolescents, and adults. Clearance and volume of distribution after adjustment for body weight were also similar.
Absorption and Distribution --Atomoxetine is rapidly absorbed after oral administration, with absolute bioavailability of about 63% in EMs and 94% in PMs. Maximal plasma concentrations (C max ) are reached approximately 1 to 2 hours after dosing.
STRATTERA can be administered with or without food. Administration of STRATTERA with a standard high-fat meal in adults did not affect the extent of oral absorption of atomoxetine (AUC), but did decrease the rate of absorption, resulting in a 37% lower C max , and delayed T max by 3 hours. In clinical trials with children and adolescents, administration of STRATTERA with food resulted in a 9% lower C max .
The steady-state volume of distribution after intravenous administration is 0.85 L/kg indicating that atomoxetine distributes primarily into total body water. Volume of distribution is similar across the patient weight range after normalizing for body weight.
At therapeutic concentrations, 98% of atomoxetine in plasma is bound to protein, primarily albumin.
Metabolism and Elimination --Atomoxetine is metabolized primarily through the CYP2D6 enzymatic pathway. People with reduced activity in this pathway (PMs) have higher plasma concentrations of atomoxetine compared with people with normal activity (EMs). For PMs, AUC of atomoxetine is approximately 10-fold and C ss,max is about 5-fold greater than EMs. Laboratory tests are available to identify CYP2D6 PMs. Coadministration of STRATTERA with potent inhibitors of CYP2D6, such as fluoxetine, paroxetine, or quinidine, results in a substantial increase in atomoxetine plasma exposure, and dosing adjustment may be necessary ( see Drug-Drug Interactions ). Atomoxetine did not inhibit or induce the CYP2D6 pathway.
The major oxidative metabolite formed, regardless of CYP2D6 status, is 4-hydroxyatomoxetine, which is glucuronidated. 4-Hydroxyatomoxetine is equipotent to atomoxetine as an inhibitor of the norepinephrine transporter but circulates in plasma at much lower concentrations (1% of atomoxetine concentration in EMs and 0.1% of atomoxetine concentration in PMs). 4-Hydroxyatomoxetine is primarily formed by CYP2D6, but in PMs, 4-hydroxyatomoxetine is formed at a slower rate by several other cytochrome P450 enzymes. N-Desmethylatomoxetine is formed by CYP2C19 and other cytochrome P450 enzymes, but has substantially less pharmacological activity compared with atomoxetine and circulates in plasma at lower concentrations (5% of atomoxetine concentration in EMs and 45% of atomoxetine concentration in PMs).
Mean apparent plasma clearance of atomoxetine after oral administration in adult EMs is 0.35 L/hr/kg and the mean half-life is 5.2 hours. Following oral administration of atomoxetine to PMs, mean apparent plasma clearance is 0.03 L/hr/kg and mean half-life is 21.6 hours. For PMs, AUC of atomoxetine is approximately 10-fold and C ss,max is about 5-fold greater than EMs. The elimination half-life of 4-hydroxyatomoxetine is similar to that of N-desmethylatomoxetine (6 to 8 hours) in EM subjects, while the half-life of N-desmethylatomoxetine is much longer in PM subjects (34 to 40 hours).
Atomoxetine is excreted primarily as 4-hydroxyatomoxetine- O -glucuronide, mainly in the urine (greater than 80% of the dose) and to a lesser extent in the feces (less than 17% of the dose). Only a small fraction of the STRATTERA dose is excreted as unchanged atomoxetine (less than 3% of the dose), indicating extensive biotransformation.
Special Populations
Hepatic insufficiency --Atomoxetine exposure (AUC) is increased, compared with normal subjects, in EM subjects with moderate (Child-Pugh Class B) (2-fold increase) and severe (Child-Pugh Class C) (4-fold increase) hepatic insufficiency. Dosage adjustment is recommended for patients with moderate or severe hepatic insufficiency ( see DOSAGE AND ADMINISTRATION ).
Renal insufficiency --EM subjects with end stage renal disease had higher systemic exposure to atomoxetine than healthy subjects (about a 65% increase), but there was no difference when exposure was corrected for mg/kg dose. STRATTERA can therefore be administered to ADHD patients with end stage renal disease or lesser degrees of renal insufficiency using the normal dosing regimen.
Geriatric --The pharmacokinetics of atomoxetine have not been eva luated in the geriatric population.
Pediatric --The pharmacokinetics of atomoxetine in children and adolescents are similar to those in adults. The pharmacokinetics of atomoxetine have not been eva luated in children under 6 years of age.
Gender --Gender did not influence atomoxetine disposition.
Ethnic origin --Ethnic origin did not influence atomoxetine disposition (except that PMs are more common in Caucasians).
Drug-Drug Interactions
CYP2D6 activity and atomoxetine plasma concentration --Atomoxetine is primarily metabolized by the CYP2D6 pathway to 4-hydroxyatomoxetine. In EMs, inhibitors of CYP2D6 increase atomoxetine steady-state plasma concentrations to exposures similar to those observed in PMs. Dosage adjustment of STRATTERA in EMs may be necessary when coadministered with CYP2D6 inhibitors, e.g., paroxetine, fluoxetine, and quinidine ( see Drug Interactions under PRECAUTIONS ). In vitro studies suggest that coadministration of cytochrome P450 inhibitors to PMs will not increase the plasma concentrations of atomoxetine.
Effect of atomoxetine on P450 enzymes --Atomoxetine did not cause clinically important inhibition or induction of cytochrome P450 enzymes, including CYP1A2, CYP3A, CYP2D6, and CYP2C9.
Albuterol --Albuterol (600 mcg iv over 2 hours) induced increases in heart rate and blood pressure. These effects were potentiated by atomoxetine (60 mg BID for 5 days) and were most marked after the initial coadministration of albuterol and atomoxetine ( see Drug-Drug Interactions under PRECAUTIONS ).
Alcohol --Consumption of ethanol with STRATTERA did not change the intoxicating effects of ethanol.
Desipramine --Coadministration of STRATTERA (40 or 60 mg BID for 13 days) with desipramine, a model compound for CYP2D6 metabolized drugs (single dose of 50 mg), did not alter the pharmacokinetics of desipramine. No dose adjustment is recommended for drugs metabolized by CYP2D6.
Methylphenidate --Coadministration of methylphenidate with STRATTERA did not increase cardiovascular effects beyond those seen with methylphenidate alone.
Midazolam --Coadministration of STRATTERA (60 mg BID for 12 days) with midazolam, a model compound for CYP3A4 metabolized drugs, (single dose of 5 mg), resulted in 15% increase in AUC of midazolam. No dose adjustment is recommended for drugs metabolized by CYP3A.
Drugs highly bound to plasma protein --In vitro drug-displacement studies were conducted with atomoxetine and other highly-bound drugs at therapeutic concentrations. Atomoxetine did not affect the binding of warfarin, acetylsalicylic acid, phenytoin, or diazepam to human albumin. Similarly, these compounds did not affect the binding of atomoxetine to human albumin.
Drugs that affect gastric pH --Drugs that elevate gastric pH (magnesium hydroxide/aluminum hydroxide, omeprazole) had no effect on STRATTERA bioavailability.
CLINICAL STUDIES
The effectiveness of STRATTERA in the treatment of ADHD was established in 6 randomized, double-blind, placebo-controlled studies in children, adolescents, and adults who met Diagnostic and Statistical Manual 4 th edition (DSM-IV) criteria for ADHD ( see INDICATIONS AND USAGE ).
Children and Adolescents
The effectiveness of STRATTERA in the treatment of ADHD was established in 4 randomized, double-blind, placebo-controlled studies of pediatric patients (ages 6 to 18). Approximately one-third of the patients met DSM-IV criteria for inattentive subtype and two-thirds met criteria for both inattentive and hyperactive/impulsive subtypes ( see INDICATIONS AND USAGE ).
Signs and symptoms of ADHD were eva luated by a comparison of mean change from baseline to endpoint for STRATTERA- and placebo-treated patients using an intent-to-treat analysis of the primary outcome measure, the investigator administered and scored ADHD Rating Scale-IV-Parent Version (ADHDRS) total score including hyperactive/impulsive and inattentive subscales. Each item on the ADHDRS maps directly to one symptom criterion for ADHD in the DSM-IV.
In Study 1, an 8-week randomized, double-blind, placebo-controlled, dose-response, acute treatment study of children and adolescents aged 8 to 18 (N=297), patients received either a fixed dose of STRATTERA (0.5, 1.2, or 1.8 mg/kg/day) or placebo. STRATTERA was administered as a divided dose in the early morning and late afternoon/early evening. At the 2 higher doses, improvements in ADHD symptoms were statistically significantly superior in STRATTERA-treated patients compared with placebo-treated patients as measured on the ADHDRS scale. The 1.8-mg/kg/day STRATTERA dose did not provide any additional benefit over that observed with the 1.2-mg/kg/day dose. The 0.5-mg/kg/day STRATTERA dose was not superior to placebo.
In Study 2, a 6-week randomized, double-blind, placebo-controlled, acute treatment study of children and adolescents aged 6 to 16 (N=171), patients received either STRATTERA or placebo. STRATTERA was administered as a single dose in the early morning and titrated on a weight-adjusted basis according to clinical response, up to a maximum dose of 1.5 mg/kg/day. The mean final dose of STRATTERA was approximately 1.3 mg/kg/day. ADHD symptoms were statistically significantly improved on STRATTERA compared with placebo, as measured on the ADHDRS scale. This study shows that STRATTERA is effective when administered once daily in the morning.
In 2 identical, 9-week, acute, randomized, double-blind, placebo-controlled studies of children aged 7 to 13 (Study 3, N=147; Study 4, N=144), STRATTERA and methylphenidate were compared with placebo. STRATTERA was administered as a divided dose in the early morning and late afternoon (after school) and titrated on a weight-adjusted basis according to clinical response. The maximum recommended STRATTERA dose was 2.0 mg/kg/day. The mean final dose of STRATTERA for both studies was approximately 1.6 mg/kg/day. In both studies, ADHD symptoms statistically significantly improved more on STRATTERA than on placebo, as measured on the ADHDRS scale.
Examination of population subsets based on gender and age (<12 and 12 to 17) did not reveal any differential responsiveness on the basis of these subgroupings. There was not sufficient exposure of ethnic groups other than Caucasian to allow exploration of differences in these subgroups.
Adults
The effectiveness of STRATTERA in the treatment of ADHD was established in 2 randomized, double-blind, placebo-controlled clinical studies of adult patients, age 18 and older, who met DSM-IV criteria for ADHD.
Signs and symptoms of ADHD were eva luated using the investigator-administered Conners Adult ADHD Rating Scale Screening Version (CAARS), a 30-item scale. The primary effectiveness measure was the 18-item Total ADHD Symptom score (the sum of the inattentive and hyperactivity/impulsivity subscales from the CAARS) eva luated by a comparison of mean change from baseline to endpoint using an intent-to-treat analysis.
In 2 identical, 10-week, randomized, double-blind, placebo-controlled acute treatment studies (Study 5, N=280; Study 6, N=256), patients received either STRATTERA or placebo. STRATTERA was administered as a divided dose in the early morning and late afternoon/early evening and titrated according to clinical response in a range of 60 to 120 mg/day. The mean final dose of STRATTERA for both studies was approximately 95 mg/day. In both studies, ADHD symptoms were statistically significantly improved on STRATTERA, as measured on the ADHD Symptom score from the CAARS scale.
Examination of population subsets based on gender and age (<42 and >/=42) did not reveal any differential responsiveness on the basis of these subgroupings. There was not sufficient exposure of ethnic groups other than Caucasian to allow exploration of differences in these subgroups.
INDICATIONS AND USAGE
STRATTERA is indicated for the treatment of Attention-Deficit/Hyperactivity Disorder (ADHD).
The effectiveness of STRATTERA in the treatment of ADHD was established in 2 placebo-controlled trials in children, 2 placebo-controlled trials in children and adolescents, and 2 placebo-controlled trials in adults who met DSM-IV criteria for ADHD ( see CLINICAL STUDIES ).
A diagnosis of ADHD (DSM-IV) implies the presence of hyperactive-impulsive or inattentive symptoms that cause impairment and that were present before age 7 years. The symptoms must be persistent, must be more severe than is typically observed in individuals at a comparable level of development, must cause clinically significant impairment, e.g., in social, academic, or occupational functioning, and must be present in 2 or more settings, e.g., school (or work) and at home. The symptoms must not be better accounted for by another mental disorder. For the Inattentive Type, at least 6 of the following symptoms must have persisted for at least 6 months: lack of attention to details/careless mistakes, lack of sustained attention, poor listener, failure to follow through on tasks, poor organization, avoids tasks requiring sustained mental effort, loses things, easily distracted, forgetful. For the Hyperactive-Impulsive Type, at least 6 of the following symptoms must have persisted for at least 6 months: fidgeting/squirming, leaving seat, inappropriate running/climbing, difficulty with quiet activities, "on the go," excessive talking, blurting answers, can't wait turn, intrusive. For a Combined Type diagnosis, both inattentive and hyperactive-impulsive criteria must be met.
Special Diagnostic Considerations
The specific etiology of ADHD is unknown, and there is no single diagnostic test. Adequate diagnosis requires the use not only of medical but also of special psychological, educational, and social resources. Learning may or may not be impaired. The diagnosis must be based upon a complete history and eva luation of the patient and not solely on the presence of the required number of DSM-IV characteristics.
Need for Comprehensive Treatment Program
STRATTERA is indicated as an integral part of a total treatment program for ADHD that may include other measures (psychological, educational, social) for patients with this syndrome. Drug treatment may not be indicated for all patients with this syndrome. Drug treatment is not intended for use in the patient who exhibits symptoms secondary to environmental factors and/or other primary psychiatric disorders, including psychosis. Appropriate educational placement is essential in children and adolescents with this diagnosis and psychosocial intervention is often helpful. When remedial measures alone are insufficient, the decision to prescribe drug treatment medication will depend upon the physician's assessment for the chronicity and severity of the patient's symptoms.
Long-term Use
The effectiveness of STRATTERA for long-term use, ie, for more than 9 weeks in child and adolescent patients and 10 weeks in adult patients, has not been systematically eva luated in controlled trials. Therefore, the physician who elects to use STRATTERA for extended periods should periodically reeva luate the long-term usefulness of the drug for the individual patient ( see DOSAGE AND ADMINISTRATION ).
CONTRAINDICATIONS
Hypersensitivity
STRATTERA is contraindicated in patients known to be hypersensitive to atomoxetine or other constituents of the product ( see WARNINGS ).
Monoamine Oxidase Inhibitors (MAOI)
STRATTERA should not be taken with an MAOI, or within 2 weeks after discontinuing an MAOI. Treatment with an MAOI should not be initiated within 2 weeks after discontinuing STRATTERA. With other drugs that affect brain monoamine concentrations, there have been reports of serious, sometimes fatal, reactions (including hyperthermia, rigidity, myoclonus, autonomic instability with possible rapid fluctuations of vital signs, and mental status changes that include extreme agitation progressing to delirium and coma) when taken in combination with an MAOI. Some cases presented with features resembling neuroleptic malignant syndrome. Such reactions may occur when these drugs are given concurrently or in close proximity.
Narrow Angle Glaucoma
In clinical trials, STRATTERA use was associated with an increased risk of mydriasis and therefore its use is not recommended in patients with narrow angle glaucoma.
WARNINGS
Allergic Events
Although uncommon, allergic reactions, including angioneurotic edema, urticaria, and rash, have been reported in patients taking STRATTERA.
Growth
Growth should be monitored during treatment with STRATTERA. During acute treatment studies (up to 9 weeks), STRATTERA-treated patients lost an average of 0.4 kg, while placebo patients gained an average of 1.5 kg. In a controlled trial that randomized patients to placebo or 1 of 3 atomoxetine doses, 1.3%, 7.1%, 19.3%, and 29.1% of patients lost at least 3.5% of their body weight in the placebo, 0.5, 1.2, and 1.8 mg/kg/day STRATTERA dose