|
ENTRESTO(sacubitril/valsartan tablets)
HIGHLIGHTS OF PRESCRIBING INFORMATION
These highlights do not include all the information needed to use ENTRESTO safely and effectively. See full prescribing information for ENTRESTO.
ENTRESTO™ (sacubitril and valsartan) tablets, for oral use
Initial U.S. Approval: 2015
WARNING: FETAL TOXICITY
See full prescribing information for complete boxed warning.
-
When pregnancy is detected, discontinue ENTRESTO as soon as possible. (5.1)
-
Drugs that act directly on the renin-angiotensin system can cause injury and death to the developing fetus. (5.1)
INDICATIONS AND USAGE
ENTRESTO is a combination of sacubitril, a neprilysin inhibitor, and valsartan, an angiotensin II receptor blocker, indicated to reduce the risk of cardiovascular death and hospitalization for heart failure in patients with chronic heart failure (NYHA Class II-IV) and reduced ejection fraction. (1.1)
ENTRESTO is usually administered in conjunction with other heart failure therapies, in place of an ACE inhibitor or other ARB. (1.1)
DOSAGE AND ADMINISTRATION
-
The recommended starting dose of ENTRESTO is 49/51 mg (sacubitril/valsartan) twice-daily. Double the dose of ENTRESTO after 2 to 4 weeks to the target maintenance dose of 97/103 mg (sacubitril/valsartan) twice-daily, as tolerated by the patient. (2.1)
-
Reduce the starting dose to 24/26 mg (sacubitril/valsartan) twice-daily for:
- patients not currently taking an angiotensin-converting enzyme inhibitor (ACEi) or an angiotensin II receptor blocker (ARB) or previously taking a low dose of these agents (2.2)
- patients with severe renal impairment (2.3)
- patients with moderate hepatic impairment (2.4)
Double the dose of ENTRESTO every 2 to 4 weeks to the target maintenance dose of 97/103 mg (sacubitril/valsartan) twice-daily, as tolerated by the patient. (2.2, 2.3, 2.4)
DOSAGE FORMS AND STRENGTHS
-
Film-coated tablets (sacubitril/valsartan): 24/26 mg; 49/51 mg; 97/103 mg (3)
CONTRAINDICATIONS
-
Hypersensitivity to any component. (4)
-
History of angioedema related to previous ACE inhibitor or ARB therapy. (4)
-
Concomitant use with ACE inhibitors. (4, 7.1)
-
Concomitant use with aliskiren in patients with diabetes. (4, 7.1)
WARNINGS AND PRECAUTIONS
-
Observe for signs and symptoms of angioedema and hypotension. (5.2, 5.3)
-
Monitor renal function and potassium in susceptible patients. (5.4, 5.5)
ADVERSE REACTIONS
Adverse reactions occurring ≥5% are hypotension, hyperkalemia, cough, dizziness, and renal failure. (6.1)
To report SUSPECTED ADVERSE REACTIONS, contact Novartis Pharmaceuticals Corporation at 1-888-669-6682 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
DRUG INTERACTIONS
-
Dual blockade of the renin-angiotensin system: Do not use with an ACEi, do not use with aliskiren in patients with diabetes, and avoid use with an ARB. (4, 7.1)
-
Potassium-sparing diuretics: May lead to increased serum potassium. (7.2)
-
NSAIDs: May lead to increased risk of renal impairment. (7.3)
-
Lithium: Increased risk of lithium toxicity. (7.4)
USE IN SPECIFIC POPULATIONS
-
Lactation: Breastfeeding or drug should be discontinued. (8.2)
-
Severe Hepatic Impairment: Use not recommended. (2.4, 8.6)
See 17 for PATIENT COUNSELING INFORMATION and FDA-approved patient labeling.
Revised: 8/2015
FULL PRESCRIBING INFORMATION: CONTENTS*
1 INDICATIONS AND USAGE
1.1 Heart Failure
ENTRESTO is indicated to reduce the risk of cardiovascular death and hospitalization for heart failure in patients with chronic heart failure (NYHA Class II-IV) and reduced ejection fraction.
ENTRESTO is usually administered in conjunction with other heart failure therapies, in place of an ACE inhibitor or other ARB.
2 DOSAGE AND ADMINISTRATION
2.1 Dosing
ENTRESTO is contraindicated with concomitant use of an angiotensin-converting enzyme (ACE) inhibitor. If switching from an ACE inhibitor to ENTRESTO allow a washout period of 36 hours between administration of the two drugs [see Contraindications (4) and Drug Interactions (7.1)].
The recommended starting dose of ENTRESTO is 49/51 mg twice-daily.
Double the dose of ENTRESTO after 2 to 4 weeks to the target maintenance dose of 97/103 mg twice daily, as tolerated by the patient.
2.2 Dose Adjustment for Patients Not Taking an ACE inhibitor or ARB or Previously Taking Low Doses of These Agents
A starting dose of 24/26 mg twice-daily is recommended for patients not currently taking an ACE inhibitor or an angiotensin II receptor blocker (ARB) and for patients previously taking low doses of these agents. Double the dose of ENTRESTO every 2 to 4 weeks to the target maintenance dose of 97/103 mg twice daily, as tolerated by the patient.
2.3 Dose Adjustment for Severe Renal Impairment
A starting dose of 24/26 mg twice-daily is recommended for patients with severe renal impairment (eGFR <30 mL/min/1.73 m2). Double the dose of ENTRESTO every 2 to 4 weeks to the target maintenance dose of 97/103 mg twice daily, as tolerated by the patient.
No starting dose adjustment is needed for mild or moderate renal impairment.
2.4 Dose Adjustment for Hepatic Impairment
A starting dose of 24/26 mg twice-daily is recommended for patients with moderate hepatic impairment (Child-Pugh B classification). Double the dose of ENTRESTO every 2 to 4 weeks to the target maintenance dose of 97/103 mg twice daily, as tolerated by the patient.
No starting dose adjustment is needed for mild hepatic impairment.
Use in patients with severe hepatic impairment is not recommended.
3 DOSAGE FORMS AND STRENGTHS
ENTRESTO is supplied as unscored, ovaloid, film-coated tablets in the following strengths:
ENTRESTO 24/26 mg, (sacubitril 24 mg and valsartan 26 mg) are violet white and debossed with “NVR” on one side and “LZ” on the other side.
ENTRESTO 49/51 mg, (sacubitril 49 mg and valsartan 51 mg) are pale yellow and debossed with “NVR” on one side and “L1” on the other side.
ENTRESTO 97/103 mg, (sacubitril 97 mg and valsartan 103 mg) are light pink and debossed with “NVR” on one side and “L11” on the other side.
4 CONTRAINDICATIONS
ENTRESTO is contraindicated:
-
in patients with hypersensitivity to any component
-
in patients with a history of angioedema related to previous ACE inhibitor or ARB therapy [see Warnings and Precautions (5.2)]
-
with concomitant use of ACE inhibitors. Do not administer within 36 hours of switching from or to an ACE inhibitor [see Drug Interactions (7.1)]
-
with concomitant use of aliskiren in patients with diabetes [see Drug Interactions (7.1)].
5 WARNINGS AND PRECAUTIONS
5.1 Fetal Toxicity
ENTRESTO can cause fetal harm when administered to a pregnant woman. Use of drugs that act on the renin-angiotensin system during the second and third trimesters of pregnancy reduces fetal renal function and increases fetal and neonatal morbidity and death. When pregnancy is detected, consider alternative drug treatment and discontinue ENTRESTO. However, if there is no appropriate alternative to therapy with drugs affecting the renin-angiotensin system, and if the drug is considered lifesaving for the mother, advise a pregnant woman of the potential risk to the fetus [see Use in Specific Populations (8.1)].
5.2 Angioedema
ENTRESTO may cause angioedema. In the double-blind period of PARADIGM-HF, 0.5% of patients treated with ENTRESTO and 0.2% of patients treated with enalapril had angioedema [see Adverse Reactions (6.1)]. If angioedema occurs, discontinue ENTRESTO immediately, provide appropriate therapy, and monitor for airway compromise. ENTRESTO must not be re-administered. In cases of confirmed angioedema where swelling has been confined to the face and lips, the condition has generally resolved without treatment, although antihistamines have been useful in relieving symptoms.
Angioedema associated with laryngeal edema may be fatal. Where there is involvement of the tongue, glottis or larynx, likely to cause airway obstruction, administer appropriate therapy, e.g., subcutaneous epinephrine/adrenaline solution 1:1000 (0.3 mL to 0.5 mL) and take measures necessary to ensure maintenance of a patent airway.
ENTRESTO has been associated with a higher rate of angioedema in Black than in non-Black patients.
Patients with a prior history of angioedema may be at increased risk of angioedema with ENTRESTO [see Adverse Reactions (6.1)]. ENTRESTO should not be used in patients with a known history of angioedema related to previous ACE inhibitor or ARB therapy [see Contraindications (4)].
5.3 Hypotension
ENTRESTO lowers blood pressure and may cause symptomatic hypotension. Patients with an activated renin-angiotensin system, such as volume- and/or salt-depleted patients (e.g., those being treated with high doses of diuretics), are at greater risk. In the double-blind period of PARADIGM-HF, 18% of patients treated with ENTRESTO and 12% of patients treated with enalapril reported hypotension as an adverse event [see Adverse Reactions (6.1)], with hypotension reported as a serious adverse event in approximately 1.5% of patients in both treatment arms. Correct volume or salt depletion prior to administration of ENTRESTO or start at a lower dose. If hypotension occurs, consider dose adjustment of diuretics, concomitant antihypertensive drugs, and treatment of other causes of hypotension (e.g., hypovolemia). If hypotension persists despite such measures, reduce the dosage or temporarily discontinue ENTRESTO. Permanent discontinuation of therapy is usually not required.
5.4 Impaired Renal Function
As a consequence of inhibiting the renin-angiotensin-aldosterone system (RAAS), decreases in renal function may be anticipated in susceptible individuals treated with ENTRESTO. In the double-blind period of PARADIGM-HF, 5% of patients in both the ENTRESTO and enalapril groups reported renal failure as an adverse event [see Adverse Reactions (6.1)]. In patients whose renal function depends upon the activity of the renin-angiotensin-aldosterone system (e.g., patients with severe congestive heart failure), treatment with ACE inhibitors and angiotensin receptor antagonists has been associated with oliguria, progressive azotemia and, rarely, acute renal failure and death. Closely monitor serum creatinine, and down-titrate or interrupt ENTRESTO in patients who develop a clinically significant decrease in renal function [see Use in Specific Populations (8.7) and Clinical Pharmacology (12.3)].
As with all drugs that affect the RAAS, ENTRESTO may increase blood urea and serum creatinine levels in patients with bilateral or unilateral renal artery stenosis. In patients with renal artery stenosis, monitor renal function.
5.5 Hyperkalemia
Through its actions on the RAAS, hyperkalemia may occur with ENTRESTO. In the double-blind period of PARADIGM-HF, 12% of patients treated with ENTRESTO and 14% of patients treated with enalapril reported hyperkalemia as an adverse event [see Adverse Reactions (6.1)]. Monitor serum potassium periodically and treat appropriately, especially in patients with risk factors for hyperkalemia such as severe renal impairment, diabetes, hypoaldosteronism, or a high potassium diet. Dosage reduction or interruption of ENTRESTO may be required [see Dosage and Administration (2.1)].
6 ADVERSE REACTIONS
Clinically significant adverse reactions that appear in other sections of the labeling include:
-
Angioedema [see Warnings and Precautions (5.2)]
-
Hypotension [see Warnings and Precautions (5.3)]
-
Impaired Renal Function [see Warnings and Precautions (5.4)]
-
Hyperkalemia [see Warnings and Precautions (5.5)]
6.1 Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
In the PARADIGM-HF trial, subjects were required to complete sequential enalapril and ENTRESTO run-in periods of (median) 15 and 29 days, respectively, prior to entering the randomized double-blind period comparing ENTRESTO and enalapril. During the enalapril run-in period, 1,102 patients (10.5%) were permanently discontinued from the study, 5.6% because of an adverse event, most commonly renal dysfunction (1.7%), hyperkalemia (1.7%) and hypotension (1.4%). During the ENTRESTO run-in period, an additional 10.4% of patients permanently discontinued treatment, 5.9% because of an adverse event, most commonly renal dysfunction (1.8%), hypotension (1.7%) and hyperkalemia (1.3%). Because of this run-in design, the adverse reaction rates described below are lower than expected in practice.
In the double-blind period, safety was eva luated in 4,203 patients treated with ENTRESTO and 4,229 treated with enalapril. In PARADIGM-HF, patients randomized to ENTRESTO received treatment for up to 4.3 years, with a median duration of exposure of 24 months; 3,271 patients were treated for more than one year. Discontinuation of therapy because of an adverse event during the double-blind period occurred in 450 (10.7%) of ENTRESTO treated patients and 516 (12.2%) of patients receiving enalapril.
Adverse reactions occurring at an incidence of ≥5% in patients who were treated with ENTRESTO in the double-blind period are shown in Table 1.
In the PARADIGM-HF trial, the incidence of angioedema was 0.1% in both the enalapril and ENTRESTO run-in periods. In the double-blind period, the incidence of angioedema was higher in patients treated with ENTRESTO than enalapril (0.5% and 0.2%, respectively). The incidence of angioedema in Black patients was 2.4% with ENTRESTO and 0.5% with enalapril [see Warnings and Precautions (5.2)].
Orthostasis was reported in 2.1% of patients treated with ENTRESTO compared to 1.1% of patients treated with enalapril during the double-blind period of PARADIGM-HF. Falls were reported in 1.9% of patients treated with ENTRESTO compared to 1.3% of patients treated with enalapril.
Laboratory Abnormalities
Hemoglobin and Hematocrit
Decreases in hemoglobin/hematocrit of >20% were observed in approximately 5% of both ENTRESTO- and enalapril-treated patients in the double-blind period in PARADIGM-HF.
Serum Creatinine
Increases in serum creatinine of >50% were observed in 1.4% of patients in the enalapril run-in period and 2.2% of patients in the ENTRESTO run-in period. During the double-blind period, approximately 16% of both ENTRESTO- and enalapril-treated patients had increases in serum creatinine of >50%.
Serum Potassium
Potassium concentrations >5.5 mEq/L were observed in approximately 4% of patients in both the enalapril and ENTRESTO run-in periods. During the double-blind period, approximately 16% of both ENTRESTO- and enalapril-treated patients had potassium concentrations >5.5 mEq/L.
7 DRUG INTERACTIONS
7.1 Dual Blockade of the Renin-Angiotensin-Aldosterone System
Concomitant use of ENTRESTO with an ACE inhibitor is contraindicated because of the increased risk of angioedema [see Contraindications (4)].
Avoid use of ENTRESTO with an ARB, because ENTRESTO contains the angiotensin II receptor blocker valsartan.
The concomitant use of ENTRESTO with aliskiren is contraindicated in patients with diabetes [see Contraindications (4)]. Avoid use with aliskiren in patients with renal impairment (eGFR <60 mL/min/1.73 m2).
7.2 Potassium-Sparing Diuretics
As with other drugs that block angiotensin II or its effects, concomitant use of potassium-sparing diuretics (e.g., spironolactone, triamterene, amiloride), potassium supplements, or salt substitutes containing potassium may lead to increases in serum potassium [see Warnings and Precautions (5.5)].
7.3 Nonsteroidal Anti-Inflammatory Drugs (NSAIDs) Including Selective Cyclooxygenase-2 Inhibitors (COX-2 Inhibitors)
In patients who are elderly, volume-depleted (including those on diuretic therapy), or with compromised renal function, concomitant use of NSAIDs, including COX-2 inhibitors, with ENTRESTO may result in worsening of renal function, including possible acute renal failure. These effects are usually reversible. Monitor renal function periodically.
7.4 Lithium
Increases in serum lithium concentrations and lithium toxicity have been reported during concomitant administration of lithium with angiotensin II receptor antagonists. Monitor serum lithium levels during concomitant use with ENTRESTO.
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
Risk Summary
ENTRESTO can cause fetal harm when administered to a pregnant woman. Use of drugs that act on the renin-angiotensin system during the second and third trimesters of pregnancy reduces fetal renal function and increases fetal and neonatal morbidity and death. Most epidemiologic studies examining fetal abnormalities after exposure to antihypertensive use in the first trimester have not distinguished drugs affecting the renin-angiotensin system from other antihypertensive agents. In animal reproduction studies, ENTRESTO treatment during organogenesis resulted in increased embryo-fetal lethality in rats and rabbits and teratogenicity in rabbits. When pregnancy is detected, consider alternative drug treatment and discontinue ENTRESTO. However, if there is no appropriate alternative to therapy with drugs affecting the renin-angiotensin system, and if the drug is considered lifesaving for the mother, advise a pregnant woman of the potential risk to the fetus.
The estimated background risk of major birth defects and miscarriage for the indicated population is unknown. In the U.S. general population, the estimated background risk of major birth defects and miscarriage in clinically recognized pregnancies is 2-4% and 15-20%, respectively.
Clinical Considerations
Fetal/Neonatal Adverse Reactions
Oligohydramnios in pregnant women who use drugs affecting the renin-angiotensin system in the second and third trimesters of pregnancy can result in the following: reduced fetal renal function leading to anuria and renal failure, fetal lung hypoplasia, skeletal deformations, including skull hypoplasia, hypotension, and death.
Perform serial ultrasound examinations to assess the intra-amniotic environment. Fetal testing may be appropriate, based on the week of gestation. Patients and physicians should be aware, however, that oligohydramnios may not appear until after the fetus has sustained irreversible injury. If oligohydramnios is observed, consider alternative drug treatment. Closely observe neonates with histories of in utero exposure to ENTRESTO for hypotension, oliguria, and hyperkalemia. In neonates with a history of in utero exposure to ENTRESTO, if oliguria or hypotension occurs, support blood pressure and renal perfusion. Exchange transfusions or dialysis may be required as a means of reversing hypotension and replacing renal function.
Data
Animal Data
ENTRESTO treatment during organogenesis resulted in increased embryo-fetal lethality in rats at doses ≥ 49 mg sacubitril/51 mg valsartan/kg/day (≤ 0.14 [LBQ657, the active metabolite] and 1.5 [valsartan]-fold the maximum recommended human dose [MRHD] of 97/103 mg twice-daily on the basis of the area under the plasma drug concentration-time curve [AUC]) and rabbits at doses ≥ 5 mg sacubitril/5 mg valsartan/kg/day (4-fold and 0.06-fold the MRHD on the basis of valsartan and LBQ657 AUC, respectively). ENTRESTO is teratogenic based on a low incidence of fetal hydrocephaly, associated with maternally toxic doses, which was observed in rabbits at an ENTRESTO dose of ≥ 5 mg sacubitril/5 mg valsartan/kg/day. The adverse embryo-fetal effects of ENTRESTO are attributed to the angiotensin receptor antagonist activity.
Pre- and postnatal development studies in rats at sacubitril doses up to 750 mg/kg/day (4.5-fold the MRHD on the basis of LBQ657 AUC) and valsartan at doses up to 600 mg/kg/day (0.86-fold the MRHD on the basis of AUC) indicate that treatment with ENTRESTO during organogenesis, gestation and lactation may affect pup development and survival.
8.2 Lactation
Risk Summary
There is no information regarding the presence of sacubitril/valsartan in human milk, the effects on the breastfed infant, or the effects on milk production. Sacubitril/valsartan is present in rat milk. Because of the potential for serious adverse reactions in breastfed infants from exposure to sacubitril/valsartan, advise a nursing woman that breastfeeding is not recommended during treatment with ENTRESTO.
Data
Following an oral dose (15 mg sacubitril/15 mg valsartan/kg) of [14C] ENTRESTO to lactating rats, transfer of LBQ657 into milk was observed. After a single oral administration of 3 mg/kg [14C] valsartan to lactating rats, transfer of valsartan into milk was observed.
8.4 Pediatric Use
Safety and effectiveness in pediatric patients have not been established.
8.5 Geriatric Use
No relevant pharmacokinetic differences have been observed in elderly (≥65 years) or very elderly (≥75 years) patients compared to the overall population [see Clinical Pharmacology (12.3)].
8.6 Hepatic Impairment
No dose adjustment is required when administering ENTRESTO to patients with mild hepatic impairment (Child-Pugh A classification). The recommended starting dose in patients with moderate hepatic impairment (Child-Pugh B classification) is 24/26 mg twice daily. The use of ENTRESTO in patients with severe hepatic impairment (Child-Pugh C classification) is not recommended, as no studies have been conducted in these patients [see Dosage and Administration (2.4), Clinical Pharmacology (12.3)].
8.7 Renal Impairment
No dose adjustment is required in patients with mild (eGFR 60 to 90 mL/min/1.73 m2) to moderate (eGFR 30 to 60 mL/min/1.73 m2) renal impairment. The recommended starting dose in patients with severe renal impairment (eGFR <30 mL/min/1.73 m2) is 24/26 mg twice daily [see Dosage and Administration (2.3), Warnings and Precautions (5.4) and Clinical Pharmacology (12.3)].
10 OVERDOSAGE
Limited data are available with regard to overdosage in human subjects with ENTRESTO. In healthy volunteers, a single dose of ENTRESTO 583 mg sacubitril/617 mg valsartan, and multiple doses of 437 mg sacubitril/463 mg valsartan (14 days) have been studied and were well tolerated.
Hypotension is the most likely result of overdosage due to the blood pressure lowering effects of ENTRESTO. Symptomatic treatment should be provided.
ENTRESTO is unlikely to be removed by hemodialysis because of high protein binding.
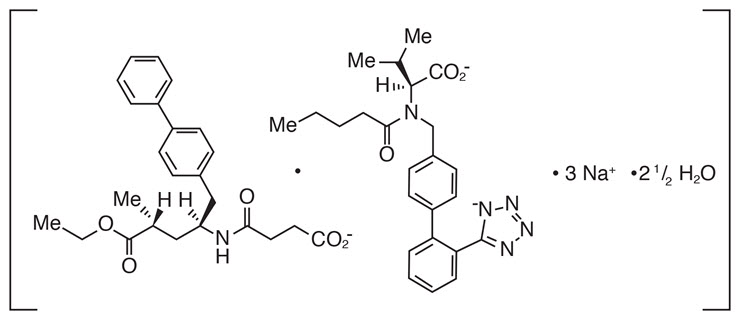
11 DESCRIPTION
ENTRESTO (sacubitril and valsartan) is a combination of a neprilysin inhibitor and an angiotensin II receptor blocker.
ENTRESTO contains a complex comprised of anionic forms of sacubitril and valsartan, sodium cations, and water molecules in the molar ratio of 1:1:3:2.5, respectively. Following oral administration, the complex dissociates into sacubitril (which is further metabolized to LBQ657) and valsartan. The complex is chemically described as Octadecasodiumhexakis(4-{[(1S,3R)-1-([1,1´-biphenyl]-4-ylmethyl)-4-ethoxy-3-methyl-4-oxobutyl]amino}-4-oxobutanoate)hexakis(N-pentanoyl-N-{[2´-(1H-tetrazol-1-id-5-yl)[1,1´-biphenyl]-4-yl]methyl}-L-valinate)—water (1/15).
Its empirical formula (hemipentahydrate) is C48H55N6O8Na3 2.5 H2O. Its molecular mass is 957.99 and its schematic structural formula is:
ENTRESTO is available as film-coated tablets for oral administration, containing 24 mg of sacubitril and 26 mg of valsartan; 49 mg of sacubitril and 51 mg of valsartan; and 97 mg of sacubitril and 103 mg of valsartan. The tablet inactive ingredients are microcrystalline cellulose, low-substituted hydroxypropylcellulose, crospovidone, magnesium stearate (vegetable origin), talc, and colloidal silicon dioxide. The film-coat inactive ingredients are hypromellose, titanium dioxide (E 171), Macrogol 4000, talc, and iron oxide red (E 172). The film-coat for the 24 mg of sacubitril and 26 mg of valsartan tablet and the 97 mg of sacubitril and 103 mg of valsartan tablet also contains iron oxide black (E 172). The film-coat for the 49 mg of sacubitril and 51 mg of valsartan tablet contains iron oxide yellow (E 172).
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
ENTRESTO contains a neprilysin inhibitor, sacubitril, and an angiotensin receptor blocker, valsartan. ENTRESTO inhibits neprilysin (neutral endopeptidase; NEP) via LBQ657, the active metabolite of the prodrug sacubitril, and blocks the angiotensin II type-1 (AT1) receptor via valsartan. The cardiovascular and renal effects of ENTRESTO in heart failure patients are attributed to the increased levels of peptides that are degraded by neprilysin, such as natriuretic peptides, by LBQ657, and the simultaneous inhibition of the effects of angiotensin II by valsartan. Valsartan inhibits the effects of angiotensin II by selectively blocking the AT1 receptor, and also inhibits angiotensin II-dependent aldosterone release.
12.2 Pharmacodynamics
The pharmacodynamic effects of ENTRESTO were eva luated after single and multiple dose administrations in healthy subjects and in patients with heart failure, and are consistent with simultaneous neprilysin inhibition and renin-angiotensin system blockade. In a 7-day valsartan-controlled study in patients with reduced ejection fraction (HFrEF), administration of ENTRESTO resulted in a significant non-sustained increase in natriuresis, increased urine cGMP, and decreased plasma MR-proANP and NT-proBNP compared to valsartan.
In a 21-day study in HFrEF patients, ENTRESTO significantly increased urine ANP and cGMP and plasma cGMP, and decreased plasma NT-proBNP, aldosterone and endothelin-1. ENTRESTO also blocked the AT1-receptor as evidenced by increased plasma renin activity and plasma renin concentrations. In PARADIGM-HF, ENTRESTO decreased plasma NT-proBNP (not a neprilysin substrate) and increased plasma BNP (a neprilysin substrate) and urine cGMP compared with enalapril.
QT Prolongation: In a thorough QTc clinical study in healthy male subjects, single doses of ENTRESTO 194 mg sacubitril/206 mg valsartan and 583 mg sacubitril/617 mg valsartan had no effect on cardiac repolarization.
Amyloid-β: Neprilysin is one of multiple enzymes involved in the clearance of amyloid-β (Aβ) from the brain and cerebrospinal fluid (CSF). Administration of ENTRESTO 194 mg sacubitril/206 mg valsartan once-daily for 2 weeks to healthy subjects was associated with an increase in CSF Aβ1-38 compared to placebo; there were no changes in concentrations of CSF Aβ1-40 or CSF Aβ1-42. The clinical relevance of this finding is unknown [see Nonclinical Toxicology (13)].
Blood Pressure: Addition of a 50 mg single dose of sildenafil to ENTRESTO at steady state (194 mg sacubitril/206 mg valsartan mg once daily for 5 days) in patients with hypertension was associated with additional blood pressure (BP) reduction (~5/4 mmHg, systolic/diastolic BP) compared to administration of ENTRESTO alone.
Co-administration of ENTRESTO did not significantly alter the BP effect of intravenous nitroglycerin.
12.3 Pharmacokinetics
Absorption
Following oral administration, ENTRESTO dissociates into sacubitril and valsartan. Sacubitril is further metabolized to LBQ657. The peak plasma concentrations of sacubitril, LBQ657, and valsartan are reached in 0.5 hours, 2 hours, and 1.5 hours, respectively. The oral absolute bioavailability of sacubitril is estimated to be ≥ 60%. The valsartan in ENTRESTO is more bioavailable than the valsartan in other marketed tablet formulations; 26 mg, 51 mg, and 103 mg of valsartan in ENTRESTO is equivalent to 40 mg, 80 mg, and 160 mg of valsartan in other marketed tablet formulations, respectively.
Following twice-daily dosing of ENTRESTO, steady |
|